
Rectus Fascial Sling
Why is it done?
- Stress urinary incontinence
- A combination of stress incontinence and detrusor over-activity of which DO is the lesser
- Involuntary urine leakage with any exertion, coughing or sneezing
- Risk factors
- More than 2 pregnancies, big babies
- Complicated deliveries, episiotomy
- Smokers
- Being overweight
- Diabetes
- Where Intrinsic Sphincter Deficiency has been proved due to a failed previous sling
- Failed previous incontinence procedures
How is it done?
- This procedure is done under a spinal/general anesthetic, as decided by the anesthetist.
- The legs will be elevated into the lithotomy position.
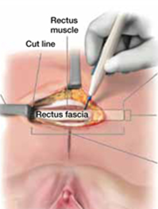
- A 10cm horizontal incision is made above the pubic bone.
- A 10-15cm X 5cm strip of rectus sheath fascia is harvested and prepared with 2 Prolene or Nylon arms
- A small incision is made in the vagina.
- The sling is placed behind the pubic bone and brought to the skin above the pubic bone, through the incision.
- The sling is placed with some tension.
- The bladder will be inspected with a cystoscopy to exclude any injuries to the bladder wall.
- The wounds are closed with dissolvable sutures and/or skin glue.
- A local anesthetic is given for pain relief.
- A urinary catheter is placed for 24hrs.
- A vaginal plug will also be placed.
- The catheter and plug will be removed early the next morning.
- The patient’s urine output will be measured each time they urinate, and the residual will be measured. (Patients will be required to do this up to 3 times.)
- If the residual amount of urine is more than 1/3 of the total bladder capacity, the patient may have to self-catheterize, until the residual volume is acceptable.
- Prophylactic antibiotics will be given to prevent infection.
Complications
- Patients will have a trial of void without catheter the next day.
- Patients will be discharged as soon as they can completely empty the bladder.
- Patients may be required to self-catheterize for a week or two.
- The sling may be loosened if placed too tight, requiring going back to the operating room.
- Patients may initially suffer from urge incontinence, but this will improve within the next 6 weeks.
- Allow 6 weeks for symptoms to stabilize.
- May also have abdominal pain with coughing and sneezing due to tension on rectus muscle
- There may be some blood in the urine. This can be remedied by drinking plenty of fluids until it clears.
Download Information Sheet
Copyright 2019 Dr Jo Schoeman
Leave a Reply
Want to join the discussion?Feel free to contribute!